Mouth Floor Reconstruction Using Tongue Flap
Tongue And Floor Of Mouth Defect Reconstruction Springerlink

Reconstruction Of The Tongue And Mouth Floor With The Myofascial Vastus Lateralis Free Flap After Cancer Ablation Semantic Scholar

A Pedicled Pectoralis Major Flap Was Used To Reconstruct A Right Download Scientific Diagram

Dentistry Dentalhygienistcup Dental Anatomy Dental Hygiene School Dentistry

18 Floor Of Mouth Reconstruction Pocket Dentistry
Three Dimensional Primary Reconstruction Of Anterior Mouth Floor And Ventral Tongue Using The Trilobed Buccinator Myomucosal Island Flap Semantic Scholar

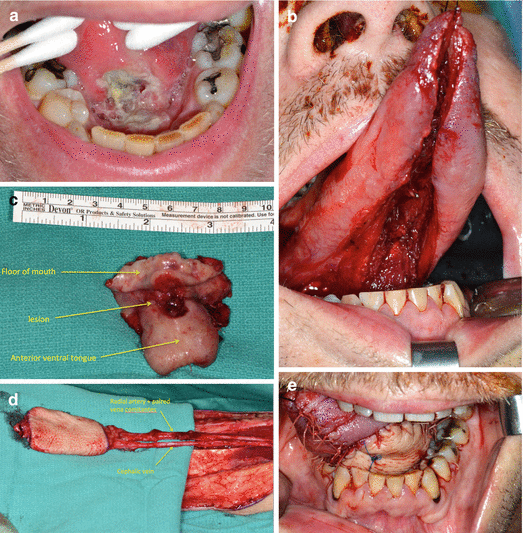
With this method reconstruction of the tongue was made the creation a large mound neotongue lateral to the mandibular arch which can easily reach the palatal arch and also was made suspension of the larynx is essential given the ablative loss of supra hyoid attachments.
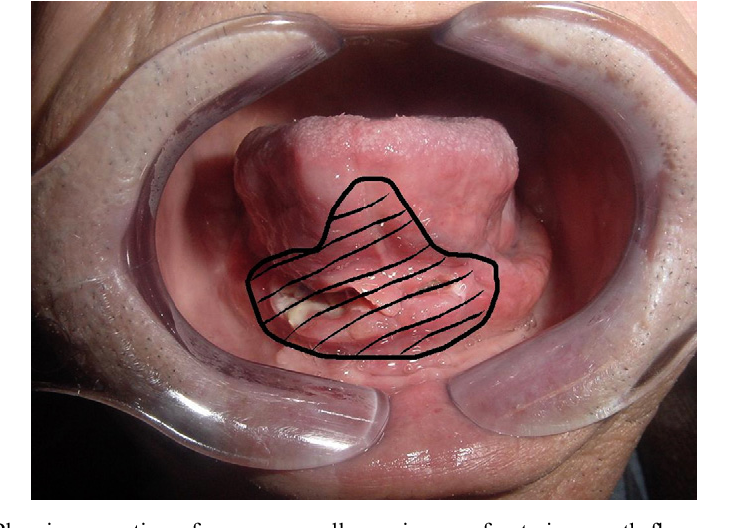
Mouth floor reconstruction using tongue flap.

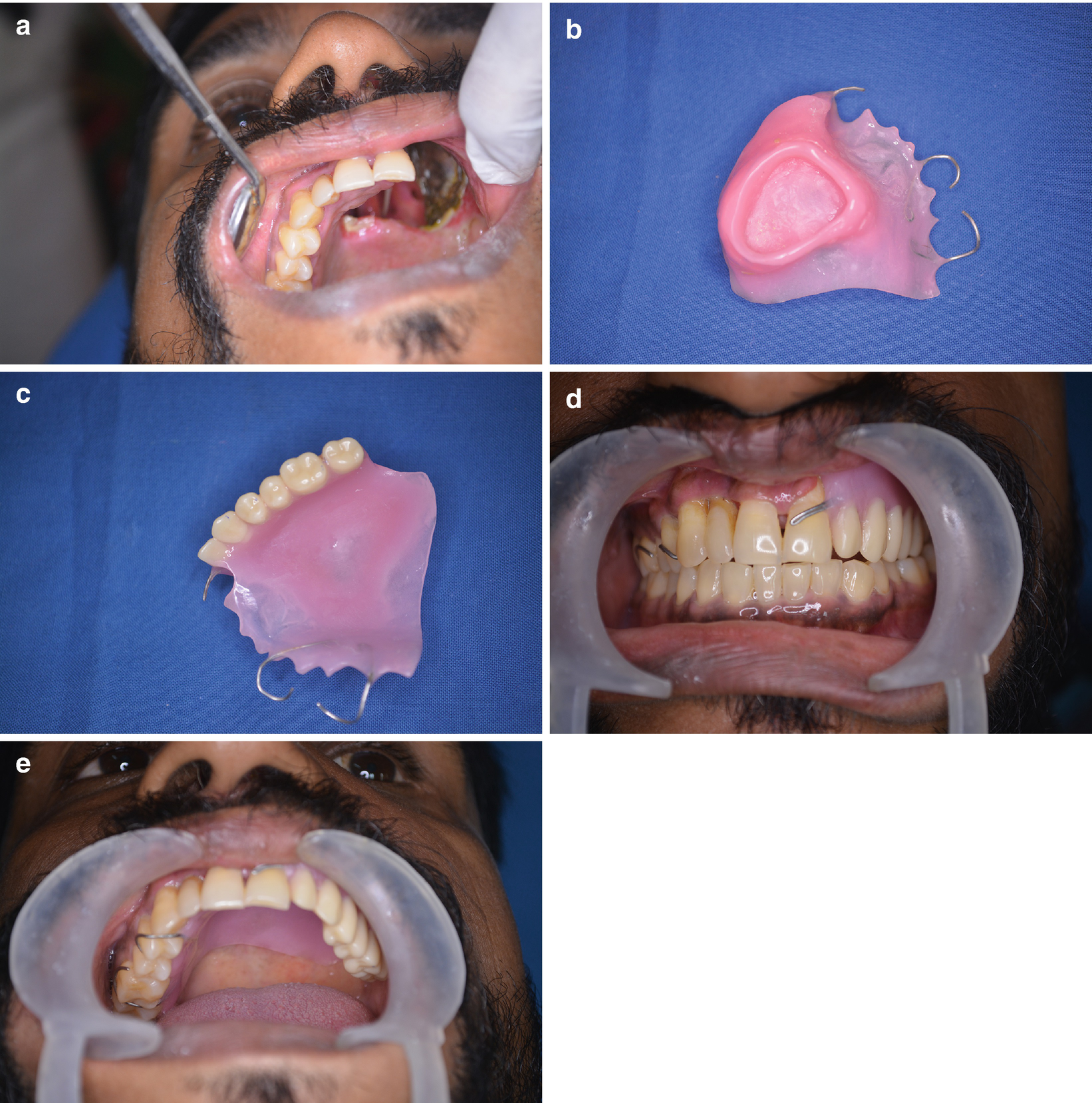
Sequence Of Oral Rehabilitation Following Resection Of An Oral Squamous Download Scientific Diagram

Floor Of Mouth Reconstruction Plastic Surgery Key

Oral Tongue And Floor Mouth Springerlink

Sensory Recovery Of Myomucosal Flap Oral Cavity Reconstructions Massarelli 2018 Head Amp Neck Wiley Online Library

Pdf Tongue Flap A Good Choice For Intraoral Reconstruction After Marginal Mandibulectomy A Single Institution Retrospective Study Of 27 Cases

Pin By Lnyx 00 On Odon In 2020 Dentistry Dental Health Temporomandibular Joint

Buccal Flap Is It Still Useful For Intraoral Reconstruction Verma 2017 Oral Surgery Wiley Online Library
Surgical Reconstruction For Cancer Of The Oral Cavity Springerlink
Https Vula Uct Ac Za Access Content Group Ba5fb1bd Be95 48e5 81be 586fbaeba29d Resection 20of 20floor 20of 20mouth 20cancers Pdf
Http Onlinelibrary Wiley Com Doi 10 1002 Hed 20722 Pdf

Rbxncxid0eylm
Dysphagia After Lip And Oral Cavity Surgery Springerlink

Endodontic Surgery Dentes

Gross Appearance Of Intraoral Flaps A Preserved Skin Structure With Download Scientific Diagram

Reconstruction Of Intraoral Defects Using Facial Artery Musculomucosal Flap British Journal Of Plastic Surgery

Submucosal Squamous Cell Carcinoma Of The Oral Tongue Presenting As Lingual Abscess

Mobilisation Second Surgery Of The Tongue Following Oral Floor Cancer Surgery Boffano 2019 Oral Surgery Wiley Online Library
About Tongue Cancer Tongue Cancer Cancer Research Uk

The Intra Oral Application Of A Skin Regeneration System In The Rehabilitation Of Post Operative Cancer Patients With Tongue Tethering A Technical Note Farrier 2017 Oral Surgery Wiley Online Library

Eradication Of Hairy Mouth After Oncological Resection Of The Tongue And Floor Mouth Using A Diode Laser 808 Nm Postoperative Pain Assessment Using Thermal Infrared Imaging Scarano 2019 Lasers

Pdf Management Of Chemical Burn In Oral Cavity

Pmmc Flap Revisited And Its Clinical Outcome In 150 Patients Springerlink

Lingual Frenectomy Wikipedia

Welcome To Our Premises In 2020 Hospital Facility Dental
Source : pinterest.com
